Perspectives
























Designing with dignity: LEO A DALY’s partnership with Tunnel to Towers to end veteran homelessness
LEO A DALY is partnering with the Tunnel to Towers Foundation to help end veteran homelessness through the development of Veterans Villages—permanent, supportive housing communities designed as true homes. Learn how our dignity-driven design approach, from adaptive reuse to ground-up development, is helping veterans rebuild stability, independence, and a sense of belonging.
Life science laboratory conversion: Five Questions with Greg McClure
Discover how existing office buildings can be transformed into high-performance life sciences labs. Learn from Greg McClure, LEO A DALY’s director of life science & education, as he explains the technical, operational, and infrastructure challenges of office-to-lab conversions. Find out what makes a building a viable candidate, how emerging technologies are reshaping lab design, and why early, comprehensive planning is essential for success in today's fast-paced real estate market.
Adaptive reuse as placemaking: Designing the future workplace from what already exists
Adaptive reuse is reshaping the future workplace—turning underperforming office buildings into vibrant, mixed-use destinations that restore urban vitality. This article explores how placemaking strategies (street-level activation, permeability, greenery, and shared amenities) can transform existing structures into social infrastructure, with 20 Massachusetts Ave NW in Washington, D.C. as a case study. By designing within what already exists, cities and developers can create more engaging, sustainable, and community-centered workplaces.
Project Highlight: Kona Village, A Rosewood Resort
Reimagined on Hawaii Island’s Kona Coast, Kona Village, A Rosewood Resort blends luxury hospitality with environmental stewardship and deep respect for place. Designed to touch the land lightly, the 83‑acre resort integrates freestanding guest hales, renewable energy, water reuse systems, and cultural preservation to create a resilient, net‑positive retreat rooted in the spirit of Hawaiʻi.
Maximizing return on investment of industrial facilities: Five Questions with Michael Schmidt
For high‑volume industrial and food distribution facilities, building design plays a critical role in operational efficiency and long‑term return on investment. In this interview, LEO A DALY Industrial Market Sector Leader Michael Schmidt explores how integrated, human‑centered, and future‑ready design strategies—from cold storage optimization to workforce safety, flexibility, and resilience—can improve daily operations and position industrial facilities for the demands of tomorrow.
Read about the engineering behind Hennepin County’s net zero-capable Public Safety Services Headquarters
Designed to operate 24/7 and achieve net zero energy, the Hennepin County Sheriff’s Office Public Safety Services Headquarters demonstrates how advanced engineering can support resilient, high‑performance public safety facilities. Learn how geothermal energy, heat recovery systems, solar power, and integrated sustainability strategies came together to make this complex building net zero‑capable.
Planning the critical access care center of the future: Five questions with Larry Crane
Rural critical access hospitals are being asked to do more with fewer resources. In this interview, LEO A DALY Healthcare Market Sector Leader Larry Crane shares how flexible, future‑ready design can help rural facilities adapt to changing care needs, improve efficiency, and better serve their communities—now and in the years ahead.
Designing a net zero building for all day, every day
Hennepin County, Minnesota, needed an energy efficient, wellness-forward space for sheriff’s deputies to train, perform administrative tasks and meet with the public. LEO A DALY provided a daylight-filled design keeping both security and wellness in mind while delivering net zero energy under continuous operation.
Insights: UCLA’s hybrid operating room
Using insights from the post-occupancy of a hybrid operating room at UCLA Ronald Reagan Medical Center, Health & Wellness market sector leader Sarvine Ashkan explains how thoughtful design advances performance, safety and workflow in complex surgical environments.
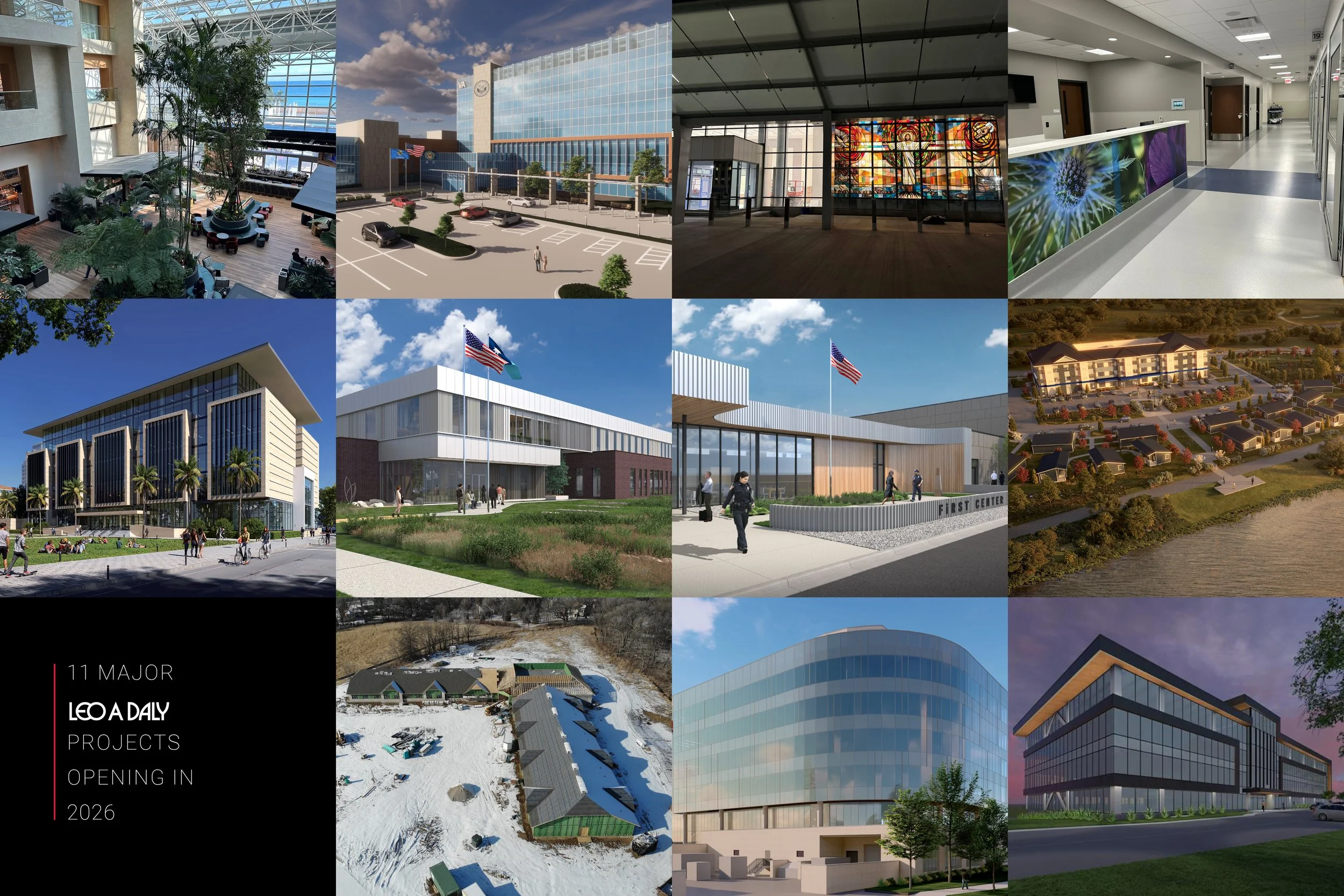
Designing the future: 11 LEO A DALY projects opening in 2026
Our architects, engineers, and designers are at the forefront of shaping communities, with a diverse portfolio of projects set to open this year. From state-of-the-art healthcare facilities that advance patient care to reimagined hospitality destinations that set new standards for luxury, each project exemplifies our belief in the power of the built environment to enrich lives.
Giving voice to all stakeholders in civic design: 5 questions with Anya Grant
Civic projects are all about the public. Universities, libraries, city halls: These institutions are for people, so the design should accommodate the needs of the people. In this interview, LEO A DALY’s Anya Grant, a civic market sector leader, shares strategies for reaching into all corners of the community to gather insight.
The inspiration behind “Taking Flight”
Enrique Greenwell and Ryan Christensen discuss the creative ideation behind the concept of converting airplane fuselages into luxury suites. The concept, “Taking Flight,” was recently featured in Forbes.
Building future-proofed technology infrastructure: Five Questions with Cody Largent
Technology Engineering Lead Cody Largent specializes in equipping buildings with the proper technology and infrastructure to ensure the facility lasts. In this edition of 5 Questions, he explains how he works with clients to find the right technological solutions.
Preserving civic architecture on a budget: Five Questions with Michael Bjornberg
Historic Preservation expert Michael Bjornberg, FAIA, skillfully navigates regulatory requirements to perform historic preservation work that meets a building owner’s needs. In this edition of 5 Questions, he talks about how to do this work on public projects, even when budgets are tight.
How public safety facilities improve wellbeing among first responders
Public safety personnel face unique physical and mental challenges. Public Safety Market Sector Leader Todd LaVold explores how thoughtful design of facilities for police officers, firefighters, and EMS can significantly improve their wellbeing, performance and retention.
Reenvisioning an historic City Hall: Five Questions with Irena Savakova
In this Five Questions interview, global design principal Irena Savakova discusses the role of placemaking and history in the reimagining of Alexandria City Hall and Market Square. A renovation project, necessitated by deteriorating conditions and a lack of accessibility, will reinvent and upgrade the historic structure and open space in Old Town Alexandria, Virginia.
Sustainable Design: Our commitment and plan to design responsibly for the future
At LEO A DALY, we hold the long view on sustainable design as responsible design, and that’s why we are signatories of all industry commitments on sustainability. The responsible use of resources translates to long term returns for our clients and communities through high performance buildings, improved open space, and healthy interior environments. Sustainability is a core value of LEO A DALY, and the firm has championed sustainable practices and materials across the markets it operates in.
In climate disasters, resilient design serves the entire community
By efficiently storing, managing, and distributing food resources, these centers help stabilize food availability after extreme weather events. In times of crisis, the importance of these centers cannot be overstated, as they are key to not only feeding populations but also supporting community recovery and fostering long-term environmental stewardship.
Decarbonization: Challenges and Opportunities in Reducing Embodied Carbon
As climate change urgency grows, reducing embodied carbon in buildings becomes crucial for creating a sustainable built environment, achieved by using materials with lower carbon footprints throughout their lifecycle.
Future-Proofing the Past through Adaptive Reuse
Uncover the technologies and skills needed to enable adaptive reuse that transforms old buildings into sustainable spaces.